Acute spasmodic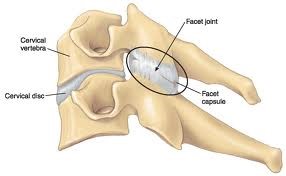 torticollis, better known as “wry neck”, is a fairly common condition characterised by a sudden loss of neck movement and severe pain. It will ordinarily occur as a result of prolonged positioning of the head or neck in an abnormal position, or perhaps an unorthodox movement associated with a sharp ‘catch’. The classic case everyone has heard is waking up after sleeping in an awkward position and not being able to move the neck due to pain and stiffness. The common presentation of an acute wry neck is unilateral pain (one sided), which is often combined with a distinct lack of movement in to contralateral lateral flexion (tilting away from the pain) and ipsilateral rotation (turning towards the pain).
torticollis, better known as “wry neck”, is a fairly common condition characterised by a sudden loss of neck movement and severe pain. It will ordinarily occur as a result of prolonged positioning of the head or neck in an abnormal position, or perhaps an unorthodox movement associated with a sharp ‘catch’. The classic case everyone has heard is waking up after sleeping in an awkward position and not being able to move the neck due to pain and stiffness. The common presentation of an acute wry neck is unilateral pain (one sided), which is often combined with a distinct lack of movement in to contralateral lateral flexion (tilting away from the pain) and ipsilateral rotation (turning towards the pain).
The two main types of acute wry neck are apophyseal and discogenic.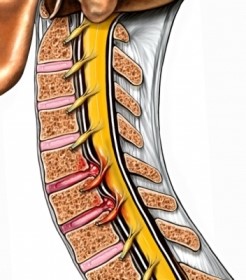 Discogenic wry neck relates to an irritation through the cervical discs that sit between the vertebrae. Much like the discs in the lower back, these can also become painful under repeated stress and occasionally place pressure on surrounding nerves in the spine. These will generally occur to the older demographics and is often associated with those prolonged periods with the head in abnormal positions e.g. an uncomfortable sleep or increasingly these days, sustained computer and mobile phone use. They present as a more diffuse pain and often build up over a longer period of time. Occasionally discogenic pain may also travel to areas like the shoulder blade or in to the arm. Discogenic wry neck will generally take longer to settle down (up to around six weeks).
Discogenic wry neck relates to an irritation through the cervical discs that sit between the vertebrae. Much like the discs in the lower back, these can also become painful under repeated stress and occasionally place pressure on surrounding nerves in the spine. These will generally occur to the older demographics and is often associated with those prolonged periods with the head in abnormal positions e.g. an uncomfortable sleep or increasingly these days, sustained computer and mobile phone use. They present as a more diffuse pain and often build up over a longer period of time. Occasionally discogenic pain may also travel to areas like the shoulder blade or in to the arm. Discogenic wry neck will generally take longer to settle down (up to around six weeks).
Apophyseal wry neck on the other hand, relates to the joints in the neck (also known as facet joints) that are crucial for rotation and tilting during normal movement. The younger population, from infants through to adolescents are much more likely to be affected by apophyseal wry neck, and are often brought about by sharp, sudden movements that result in a catching or acute restriction in the facet joints. Unlike discogenic wry neck, these tend to be more localised and once the facet joint has been released and is able to move more freely, they will settle more quickly (around 1-2 weeks).
Management
The diagnosis of acute wry neck is often after assessment by a physiotherapist or physician. Most cases of acute wry neck respond well to conservative treatment by a physiotherapist. The best approach to management is early assessment and mobilisation as opposed to resting or immobilising the area. Immobilisation for long periods will tend to stiffen the area up further and increase muscle spasm, thereby increasing the likely recovery time. Early mobilisation can be achieved through a combination of:
- Manual therapy (massage, muscle energy techniques, mobilisations)
- Postural retraining
- Motor control exercises
- Pain control (heat, pain medication, taping)
Whether you develop these symptoms over a period of time, or whether the onset is rapid and highly debilitating, be sure to be proactive in having it assessed by a physiotherapist in order to get back to doing what you love in as little time as possible.
Article by Kieran Watson
