Swimmer’s shoulder is an umbrella term covering a range of painful shoulder  overuse injuries that occur in swimmers. Being an overuse injury, it is caused by repeated trauma rather than a specific incident.
overuse injuries that occur in swimmers. Being an overuse injury, it is caused by repeated trauma rather than a specific incident.
Freestyle along with backstroke and butterfly have a much larger amount of rotation at the shoulder joint than breaststroke (The majority of injuries in the lower body occur during the breaststroke). Research has indicated that freestyle is the stroke most prone to shoulder injury.
There are various parts of the shoulder which can be injured from your swimming stroke, however this generally tends to occur in either the top or front of the joint, often as a result of compression of the soft tissue of the shoulder against bony areas such as the acromion on the top or the coracoid process in the front of the shoulder. The pain will typically be a local to the shoulder joint, however may also spread into the neck or refer into the upper arm.
Shoulder Anatomy
Your shoulder is a ball and socket joint, with a rim of cartilage that goes around the 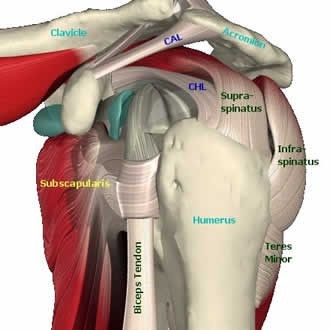 socket to make it deeper and more stable.
socket to make it deeper and more stable.
Surrounding the joint is your joint capsule, a fibrous material, with thicker parts of the capsule forming ligaments.
A number of muscles, and the tendons from these muscles, run around and over your joint. The muscles that have the most effect on your joint stability are called the rotator cuff. The ‘cuff’ is made up of four muscles which work together to help keep your shoulder centered in the socket.
What Goes Wrong in Swimmers Shoulder?
The shoulder is a very mobile joint, and being so mobile, it needs to be well controlled by the muscles and ligaments that surround the joint.
Over-training, fatigue, hypermobility, poor stroke technique, weakness, tightness, previous shoulder injury or use of hand paddles can lead to poorly controlled motion and overload of the shoulder. If this goes on, irritation and wear to the ligaments, bursa or cartilage of the shoulder can occur.
Research has indicated that the shoulder joint is at its most vulnerable during sprint events and when fatigued, which often results in poor movement patterns during the stroke. The most common technical flaw is ‘elbow drop’ during the pull through phase of the stroke.
Diagnosis
Getting the correct diagnosis is very important in order to get the most appropriate treatment, and to get you back in the pool as quickly as possible. Your physiotherapist is able to run through a range of test in order to both identify the structure in the shoulder which is giving you pain as well as whether this has occurred as a result of stiffness, weakness, poor stroke or just simply over training.
Treatment
Advice and education about the nature and pathology of the condition including  tips on self-management is vital in the early stages. As with most soft tissue injuries the initial treatment involves allowing the affected area to rest and recover. Attempting to swim and train through the pain generally only results in further damage to the shoulder and ultimately a longer period out of the pool.
tips on self-management is vital in the early stages. As with most soft tissue injuries the initial treatment involves allowing the affected area to rest and recover. Attempting to swim and train through the pain generally only results in further damage to the shoulder and ultimately a longer period out of the pool.
Anti-inflammatory medication (if tolerated) maybe recommended to help reduce your pain and swelling. However, it is best to avoid anti-inflammatory drugs during the initial 48 to 72 hours when they may encourage additional bleeding.
Based on your presentation, your physiotherapist will use a range of techniques such as massage, stretching, myofascial release, taping and acupuncture or dry needling to assist in relieving pain and restoring normal joint mechanics.
Most injuries do not occur without some form of poor movement patterns. Exercises aimed at strengthening the rotator cuff, shoulder complex and correcting abhorrent biomechanics generally play a pivotal role in the later stages of rehab in preventing the injury from re-occurring once swimming re-commences.
Swimming specific training drills should be introduced prior to returning to the pool. Literature frequently refers to the ‘pull through phase’ when discussing swimmer’s shoulder. It indicates that the majority of force originates from the back. It can be assumed training the anterior muscles of the upper body to excess can be counterproductive as this can encourage force to be produced in the wrong direction as well as inhibiting thoracic extension and optimal range at the shoulder joint.
Research suggests that increasing the strength of the shoulder adductors such as the large lats muscles on the side of the trunk, helps to assist in maintaining shoulder and elbow alignment during the stroke. Compound overhead movement patterns such as push presses and jerks, will help promote both stability and strength, while simultaneously working the shoulder joint in multiple planes of motion.
There is no specific time frame for progression and return to swimming and this must be guided by both the condition of the tissue and your ability to learn correct movement patterns. It is also important to note that each progression must be carefully monitored as attempting to progress too soon to the next level can lead to re-injury and frustration.
At In Balance Physio and Pilates our physiotherapists are experienced in the types of injuries that swimmers suffer. For more specific advice about your shoulder injury, please contact us at In Balance Physio and Pilates.
