What is FAI?
In recent history, there has been increasing recognition of femoroacetabular impingement as a major cause of hip pain and labral tears in active young to middle aged adults. It has also been proposed as a possible cause of secondary osteoarthritis. Femoroacetabular impingement, or FAI relates to an abnormal impingement pattern in the hip joint between the acetabulum (socket) and the femoral head (ball). The hip joint is a ball and socket joint where the acetabulum creates the socket portion, and the femoral head is the ball. With articular cartilage covering both, they are designed to conform well to each other, allowing smooth, low friction movement of the hip. When this symmetry is compromised it can result in pain and reduced function.
What causes FAI?
The risk factors for development of FAI are not well understood 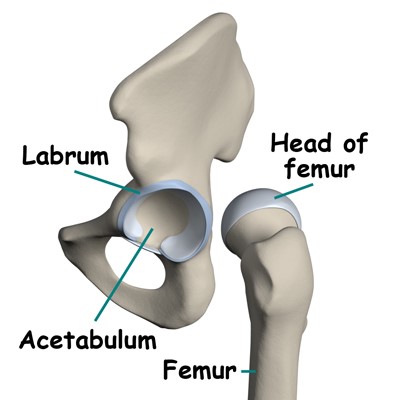 but several factors such as bone remodelling due to repeated friction, hip-shape abnormalities, irregular biomechanics and muscle imbalance during sport have all been proposed to contribute. There is also evidence that developmental abnormalities of the hip as a child may lead to symptoms later in life.
but several factors such as bone remodelling due to repeated friction, hip-shape abnormalities, irregular biomechanics and muscle imbalance during sport have all been proposed to contribute. There is also evidence that developmental abnormalities of the hip as a child may lead to symptoms later in life.
Symptoms
FAI presents often as groin pain or frontal hip pain and less commonly to the side of the hip and in the buttock. Pain is often accompanied by reduced range in multiple directions, but the more common restrictions are into flexion and internal rotation. Pain can be reported as a dull ache or quite sharp, and in some cases there may be reports of clicking or giving way in the hip.
Types of FAI
There are commonly three types of FAI. These include:
- CAM type: commonly found in active adolescents,
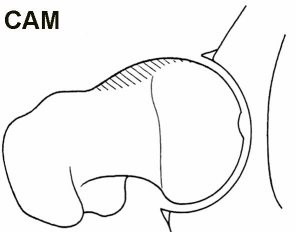 CAM type FAI involves a widening of the femoral neck or misshapen femoral head which will cause abrasion on the acetabulum
CAM type FAI involves a widening of the femoral neck or misshapen femoral head which will cause abrasion on the acetabulum
- Pincer type: a less seen version, more common
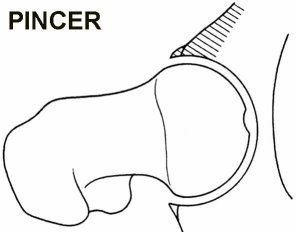 in middle aged women, pincer type FAI is an overcoverage of the socket joint around the head of the femur. I.e. new bone forms at the edge of the socket.
in middle aged women, pincer type FAI is an overcoverage of the socket joint around the head of the femur. I.e. new bone forms at the edge of the socket.
- Mixed type: a combination of the two presentations above. Impingement is rarely either CAM or pincer type in isolation
Diagnosis
Diagnosis is often made through a detailed subjective and physical examination, using common hip impingement testing such as hip flexion, adduction and internal rotation (FADIR’s test) or less commonly flexion, hip abduction and external rotation (FABER’s test) to elicit a painful response.
To further confirm or rule out FAI, radiography techniques such as an X-ray can be performed initially, followed by MRI or CT scan if deemed necessary.
What are the management options?
Conservative treatment should always be the first option to help settle FAI. Anti-inflammatories or pain medication can be a helpful adjunct in the acute stage to settle down any inflammatory processes. Physiotherapy has been shown to be effective at reducing pain and improving function in FAI populations. Physio management revolves around:
- manual therapy aimed at restoring joint range and soft tissue pliability
- exercise-based rehabilitation program focusing on increasing flexibility, strength and control in the hip and gluteal global and stabilising muscles
- activity modification is key in settling down symptoms whilst other streams of treatment are performed. Common modification may be avoiding prolonged sitting, deep squats, pivoting, crossing the legs or high impact sports such as running or soccer. Instead cross-training activities such as swimming or walking may be indicated.
When conservative treatment with a physiotherapist is not effective, referral onwards to an orthopaedic surgeon is recommended. Surgical correction involves altering the shape of any hip abnormalities around the femoral neck or acetabulum to normalise joint range. If you feel that your symptoms closely follow those described above, come in and see a physiotherapist at In Balance Physio & Pilates for a detailed musculoskeletal assessment.
Article by Kieran Watson
